Last Reviewed: 01 Aug 2024
The exact prevalence of ARFID in the general population is unknown, with studies reporting from 0.3% to 15.5% of the population in children (Kurtz et al., 2015; Goncalves et al., 2019; Dinkler et al., 2022; Sanchez‐Cerezo, et al, 2023), adolescents (Van Buuren et al., 2023) and adults (Hay et al., 2017; Hilbert, et al., 2021: D’Adamo et al., 2023).
Current prevalence rates are predominantly based on retrospective data, and it is anticipated that prevalence rates will change once prospective data is obtained. An Australian study, Hay et al (2017), demonstrated that ARFID may be just as common as other, more widely known eating disorders based on a population-based survey, with 1 in 300, that is, 0.3% people in Australia being affected.
Prevalence estimates from clinical eating disorder (ED) populations range from 1.5% to 64% (Zickgraf et al, 2019; Nicely et al., 2014, Bourne, et al, 2020).
13.8% prevalence in USA/Canadian eating disorder health care settings in 8–18-year-olds (Fisher et al., 2014).
5-24% prevalence in eating disorder settings (Norris et al., 2016).
1.5% - 8% paediatric gastroenterology (Eddy et al., 2015; Murray & Calabrese, 2022).
3.7% paediatric gynaecology (Goldberg et al., 2020).
6.3% in adult neuro-gastroenterology (Murray et al., 2020).
Among a clinical child and adolescent group (N=261), Watts et al (2023) found an equal sex ratio of ARFID, including among the three drivers of ARFID (sensory-based avoidance, lack of inter- est, and fear of adverse consequences).
A retrospective chart review found ARFID to be equally common in males and females in infancy and early childhood, but has a male predominance in middle childhood when it is often co-occurringbid with autism (Nicely et al., 2014).
The reported rates of ARFID may differ widely for several reasons. Following the new ARFID diagnostic criteria in the DSM-5-TR (American Psychiatric Association, 2022), Coglan & Otasowie (2018) note:
“Current prevalence rates have been calculated using retrospective data to assign patients to a diagnosis of ARFID. It is not unlikely that the prevalence may change when ARFID diagnosis becomes more stable in terms of recognition (e.g., through prospective surveillance and population studies)”.
In addition to this, health professionals may lack the knowledge and experience to confidently differentiate ARFID from picky eating (Zickgraf et al, 2019) resulting in higher rates of ARFID being identified. Also, the DSM-5 criteria (American Psychiatric Association, 2013) do not include clear definitions of weight or nutritional requirements for a diagnosis of ARFID; while only recently, DSM-5-TR (American Psychiatric Association, 2022) clarified that a diagnosis of ARFID can be made when eating difficulties affect physical health or lead to psychosocial impairment (Archibald & Bryant-Waugh, 2023).
Care Cooney et al (2018) reported ARFID child and adolescent presentations in tertiary settings had a high prevalence of premorbid history of picky eating, nausea, and a reported specific trigger for their feeding/ eating disturbance before diagnosis.
Assessment involving a thorough history of eating, physical symptoms, medical problems, and details around the eating/feeding disturbance onset is ESSENTIAL.
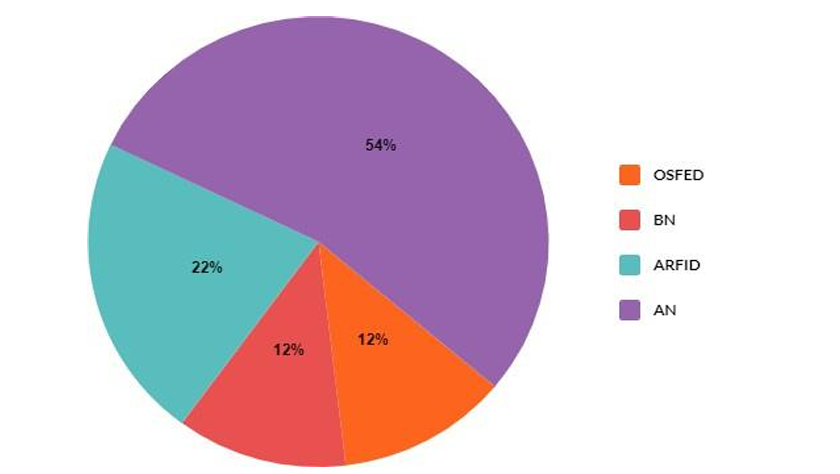
DSM-5-TR Diagnostic presentations of Adolescent Eating Disorders in Tertiary Eating Disorders Care (Hay et al., 2023).
“Due to people presenting to a range of clinical settings, the ongoing differences among health care professionals surrounding knowledge and awareness of ARFID needs to be actively addressed. The detection of possible ARFID cases can and should, be made by all health care professionals from primary through to tertiary care, and not limited to a particular subgroup of specialist practitioners” (Eddy et al., 2019).
“Ongoing awareness raising and training on the current conceptualisation of ARFID remains strongly indicated” (Archibald & Bryant-Waugh, 2023).
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders, fifth edition (DSM-5). Washington: American Psychiatric Association.
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders, fifth edition, text revision (DSM-5-TR). Washington: American Psychiatric Association.
Archibald, T., & Bryant‐Waugh, R. (2023). Current evidence for avoidant restrictive food intake disorder: Implications for clinical practice and future directions. JCPP Advances, e12160. doi: 10.1002/jcv2.12160
Bourne, L., Bryant-Waugh, R., Cook, J., & Mandy, W. (2020). Avoidant/restrictive food intake disorder: A systematic scoping review of the current literature. Psychiatry Research, 288, 112961. doi: 10.1016/j.psychres.2020.112961
Coglan, L., & Otasowie, J. (2019). Avoidant/restrictive food intake disorder: what do we know so far? British Journal Psychological Advances, 25(2), 90-98. doi:10.1192/bja.2018.48
Cooney, M., Lieberman, M., Guimond, T., & Katzman, D. K. (2018). Clinical and psychological features of children and adolescents diagnosed with avoidant/restrictive food intake disorder in a pediatric tertiary care eating disorder program: a descriptive study. Journal of Eating Disorders, 6(1), 1-8. doi: 10.1186/s40337-018-0193-3
D’Adamo, L., Smolar, L., Balantekin, K., Taylor, C. B., Wilfley, D., & Fitzsimmons-Craft, E. (2023). Prevalence, Char- acteristics, and Correlates of Avoidant/Restrictive Food Intake Disorder among Adult Respondents to the National Eating Disorders Association Online Screen: A Cross-Sectional Study. Research Square. doi: 10.1186/s40337-023-00939-0
Dinkler, L., Yasumitsu-Lovell, K., Eitoku, M., Fujieda, M., Suganuma, N., Hatakenaka, Y., Bryant-Waugh, R., Råstam, M., & Gillberg, C. (2022). Development of a parent-reported screening tool for avoidant/restrictive food intake disorder (ARFID): Initial validation and prevalence in 4-7-year-old Japanese children. Appetite, 168, 105735. doi: 10.1016/j.appet.2021.105735
Eddy, K. T., Thomas, J. J., Hastings, E., Edkins, K., Lamont, E., Nevins, C. M., Patterson, R. M., Murray, H. B., Bryant-Waugh, R., & Becker, A. E. (2015). Prevalence of DSM‐5 avoidant/restrictive food intake disorder in a pediatric gastroenterology healthcare network. International Journal of Eating Disorders, 48(5), 464-470. doi: 10.1002/eat.22350
Eddy, K. T., Harshman, S. G., Becker, K. R., Bern, E., Bryant‐Waugh, R., Hilbert, A., Katzman, D. K., Lawson, E. A., Manzo, L. D., Menzel, J., Micali, N., Ornstein, R., Sally, S., Serinsky, S. P., Sharp, W., Stubbs, K., Walsh, B. T., Zickgraf, H., Zucker, N., & Thomas, J. J. (2019). Radcliffe ARFID Workgroup: Toward operationalization of research diagnostic criteria and directions for the field. International Journal of Eating Disorders, 52(4), 361-366. doi: 10.1002/eat.23042
Fisher, M. M., Rosen, D. S., Ornstein, R. M., Mammel, K. A., Katzman, D. K., Rome, E. S., Callahan, S. T., Malizio, J., Kearney, S., & Walsh, B. T. (2014). Characteristics of avoidant/restrictive food intake disorder in children and adolescents: a “new disorder” in DSM-5. Journal of Adolescent Health, 55(1), 49-52. doi: 10.1016/j.jadohealth.2013.11.013
Goldberg, H. R., Katzman, D. K., Allen, L., Martin, S., Sheehan, C., Kaiserman, J., Macdonald, G., & Kives, S. (2020). The Prevalence of Children and Adolescents at Risk for Avoidant Restrictive Food Intake Disorder in a Pediatric and Adolescent Gynecology Clinic. Journal of Pediatric and Adolescent Gynecology, 33(5), 466-469. doi: 10.1016/j.jpag.2020.06.004
Gonçalves, S., Vieira, A. I., Machado, B. C., Costa, R., Pinheiro, J., & Conceiçao, E. (2019). Avoidant/restrictive food intake disorder symptoms in children: Associations with child and family variables. Children's Health Care, 48(3), 301 313. doi: 10.1080/02739615.2018.1532796
Hay, P., Mitchison, D., Collado, A. E. L., González-Chica, D. A., Stocks, N., & Touyz, S. (2017). Health-related quality of life of eating disorders, including avoidant/restrictive food intake disorder (ARFID), in the Australian population. Journal of Eating Disorders, 5, 21. doi: 10.1186/s40337-017-0149-z
Hay, P., Aouad, P., Le, A., Marks, P., Maloney, D., Touyz, S., & Maguire, S. (2023). Epidemiology of eating disorders: population, prevalence, disease burden and quality of life informing public policy in Australia—a rapid review. Journal of Eating Disorders, 11(1), 23. doi: 10.1186/s40337-023-00738-7
Hilbert, A., Zenger, M., Eichler, J., & Brähler, E. (2021). Psychometric evaluation of the Eating Disorders in Youth‐ Questionnaire when used in adults: Prevalence estimates for symptoms of avoidant/restrictive food intake disorder and population norms. International Journal of Eating Disorders, 54(3), 399-408. doi: 10.1002/eat.23424
Kurz, S., Van Dyck, Z., Dremmel, D., Munsch, S., & Hilbert, A. (2015). Early-onset restrictive eating disturbances in primary school boys and girls. European Child & Adolescent Psychiatry, 24, 779-785. doi: 10.1007/s00787-014-0622-z
Murray, H. B., Bailey, A. P., Keshishian, A. C., Silvernale, C. J., Staller, K., Eddy, K. T., Thomas, J. J., & Kuo, B. (2020). Prevalence and characteristics of avoidant/restrictive food intake disorder in adult neurogastroenterology patients. Clinical Gastroenterology and Hepatology, 18(9), 1995-2002. doi: 10.1016/j.cgh.2019.10.030
Murray, H. B., & Calabrese, S. (2022). Identification and management of eating disorders (including ARFID) in GI patients. Gastroenterology Clinics, 51(4), 765-783. doi: 10.1016/j.gtc.2022.07.004
Nicely, T. A., Lane-Loney, S., Masciulli, E., Hollenbeak, C. S., & Ornstein, R. M. (2014). Prevalence and characteristics of avoidant/restrictive food intake disorder in a cohort of young patients in day treatment for eating disorders. Journal of Eating Disorders, 2, 21. doi: 10.1186/s40337-014-0021-3
Norris, M. L., Spettigue, W. J., & Katzman, D. K. (2016). Update on eating disorders: current perspectives on avoidant/restrictive food intake disorder in children and youth. Neuropsychiatric Disease and Treatment, 19(12), 213 218. doi: 10.2147/NDT.S82538
Sanchez-Cerezo, J., Nagularaj, L., Gledhill, J., & Nicholls, D. (2023). What do we know about the epidemiology of avoidant/restrictive food intake disorder in children and adolescents? A systematic review of the literature. European Eating Disorders Review, 31(2), 226-246. doi: 10.1002/erv.2964
Van Buuren, L., Fleming, C. A. K., Hay, P., Bussey, K., Trompeter, N., Lonergan, A., & Mitchison, D. (2023). Correction: The prevalence and burden of avoidant/restrictive food intake disorder (ARFID) in a general adolescent population. Journal of Eating Disorders, 11(1), 148. doi: 10.1186/s40337-023-00873-1
Watts, R., Archibald, T., Hembry, P., Howard, M., Kelly, C., Loomes, R., Markham, L., Moss, H., Munuve, A., Oros, A., Siddall, A., Rhind, C., Uddin, M., Ahmad, Z., Bryant-Waugh, R., & Hübel, C. (2023). The clinical presentation of avoidant restrictive food intake disorder in children and adolescents is largely independent of sex, autism spectrum disorder and anxiety traits. eClinicalMedicine, 63, 102190. doi: 10.1016/j.eclinm.2023.102190
Zickgraf, H. F., Murray, H. B., Kratz, H. E., & Franklin, M. E. (2019). Characteristics of outpatients diagnosed with the selective/neophobic presentation of avoidant/restrictive food intake disorder. International Journal of Eating Disorders, 52(4), 367-377. doi: 10.1002/eat.23013
© 2026 InsideOut
InsideOut acknowledges the tradition of custodianship and law of the Country on which the University of Sydney and Charles Perkins Centre campus stands. We pay our respects to those who have cared and continue to care for Country. We are committed to diversifying research and eliminating inequities and discrimination in healthcare. We welcome all people regardless of age, gender, race, size, sexuality, language, socioeconomic status, location or ability.